In brief
- Ingrown hairs occur when the hair growth under the skin happens at an angle or gets blocked under the stratum corneum, often triggering a skin inflammation.
- A red itchy bump can remain simple, but throbbing pain, a warm lump, and pus suggest a follicular infection that needs medical attention.
- The temptation to “pierce” with a needle or tweezers increases the risk of scarring and secondary infection, even with approximate disinfection.
- A gentle and regular exfoliation, combined with suitable skin care, helps the hair find its way outwards again.
- Ingrown hair prevention involves choosing the depilation method, shaving quality, hydration, and reducing friction.
- When lesions multiply on the pubic area, beard, or armpits, or when a cyst swells quickly, ingrown hair treatment should be assessed to avoid progression to an abscess.

Ingrown hairs: understanding hair growth under the skin and the inflammatory reaction
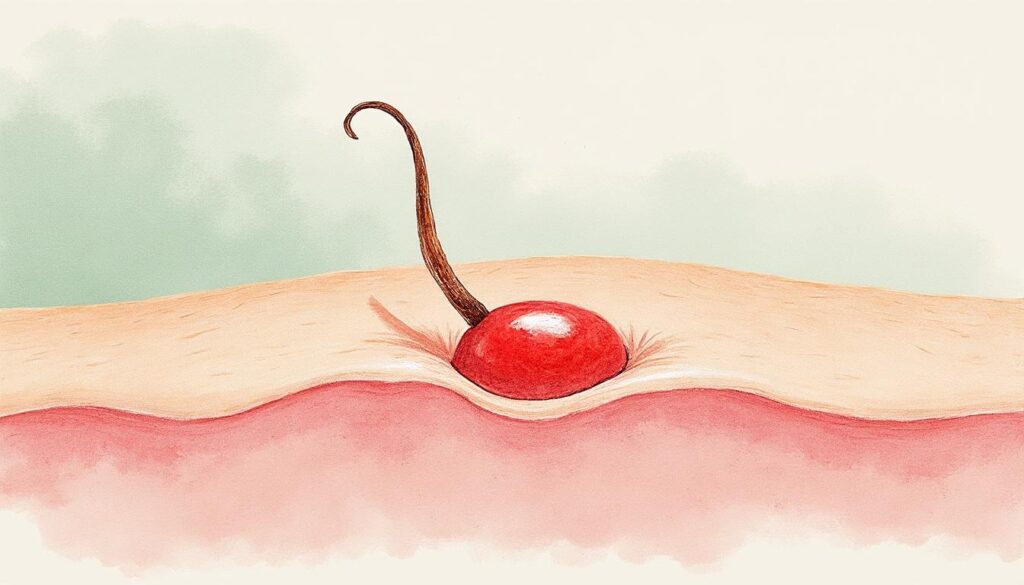
The skin functions as a barrier. It protects, regulates, and filters. A hair grows from a hair follicle and follows a precise channel to exit into the open air. When this path goes awry, the hair growth under the skin can occur laterally or curl onto itself. The hair continues to grow, but it becomes trapped under the epidermis, as if a door that’s too thick refuses to open.
The body then reacts as it knows how to against what it perceives as an attack. It sends immune cells to the site. This creates a localized skin inflammation. Visually, the area becomes red. To the touch, it may be sensitive. Some people describe a burning sensation, others an itch that makes them want to scratch.
Ingrown hairs are not limited to one area. They appear wherever hair is present, but certain locations recur often because they combine friction, moisture, or repeated shaving. The beard and neck in men are concerned, especially when shaving pulls on the hair. Legs, armpits, and arms are typical after razor or waxing. The pubic area concentrates several irritating factors. Heat and friction from underwear make the area more reactive, and inflammation becomes painful faster there.
The type of hair also matters. Thick, curly, or very bent hair can more easily fold back and “seek” the path of least resistance under the skin. Dry skin, thickened by dead cells, or conversely weakened by repeated irritation, can block the exit. The result is the same. The hair shaft remains trapped and maintains the reaction.
Sometimes an ingrown hair is silent. No bump, no pain. It stays under the skin and then frees itself with natural desquamation. In other cases, a small bump appears. The skin forms a red lump, sometimes with a visible dark spot. This spot is not “dirt” from a pore. It’s often the tip of the hair that failed to break through.
In some infants, parents sometimes notice small ingrown hairs on the scalp, especially on dry or flaky skin. The mechanism is similar, even if the context differs. Baby skin in the first weeks sheds a lot. When thick flakes accumulate, the exit of a fine hair can be hindered. Gentle cleansing and appropriate hydration are usually enough, without manipulation.
An ingrown hair is not a hair that “grows backward”. It grows, but it does not pass through the skin barrier at the right spot. This nuance changes the way to act. The useful action aims to soften the superficial layer, not to “force” deeply. This understanding naturally leads to the next question, about factors that favor or maintain the phenomenon.
Once the mechanism is understood, attention shifts to what, daily, transforms a simple regrowth incident into a recurring problem.
Why ingrown hairs return: shaving, depilation, friction, and thickened skin
The common thread in recurrences is often a repetition of the same scenario. The skin is stressed, sometimes damaged, then the hair regrows in a less supple environment. Shaving is a very frequent factor. A dull blade does not cut cleanly. It can snag, slightly break the shaft, leaving a sharper and shorter tip. When regrowing, this hair can pierce the neighboring skin rather than following its channel.
Shaving against the grain increases this risk. It gives a smoother skin sensation at the moment but cuts the hair lower. When it regrows, it must cross a sometimes thickened stratum corneum. The beard and neck are particularly concerned because the skin there is mobile and hair growth direction varies by zone. Identical shaving motions everywhere on the face don’t match this fine geography.
Depilation by waxing or tweezing can also encourage ingrown hairs. The hair is pulled out. At regrowth, it can be thinner at first, less “equipped” to cross the skin barrier. If it encounters dry skin, dead cell buildup, or irritation, it deviates. Methods creating repeated micro-traumas, especially on already sensitive skin, maintain the inflammatory environment.
The pubic area has a particularity. Hairs there are often thicker. The skin is exposed to moisture, heat, and frequent friction. Tights, tight jeans, a sports session, a long seated trip—all these create friction that irritates and thickens locally. The hair, instead of coming out straight, curls under the surface. A simple redness can then evolve faster into a deeper lesion.
Dry skin plays a subtle but powerful role. When skin hydration is insufficient, the stratum corneum becomes less flexible. It acts more like a “lid.” Regrowth then happens against mechanical resistance. Regular moisturizing treatments have a very concrete effect. They reduce this resistance and make the exit easier.
Certain profiles are more exposed. Dense hair mechanically multiplies the chances of ingrowth. Curly or kinky hairs, whether beard hairs or scalp hair on a shaved head, tend to curl and re-enter the epidermis more. On the scalp, very regular shaving with a dull blade increases the probability of ingrown hairs, especially if the scalp is covered with flakes or sebum.
Recurrences are not inevitable. They often express a duo. A depilation or shaving technique that weakens the exit, and skin that defends itself by thickening. The work is therefore at two levels. Change the movement, and improve the skin surface condition. This logic naturally leads to signs that help distinguish a simple bump from a situation tipping toward infection.
When the skin becomes warm, pain increases, or a white spot appears, the question is no longer just “why” but “how to prevent worsening.”
Recognizing skin inflammation and follicular infection: useful signs, traps, and guidelines
A skin inflammation around an ingrown hair can remain moderate. The area is red, slightly swollen, sometimes itchy. It looks like a small bump after shaving. It can calm down in a few days, especially if the area is no longer stressed. In this context, the skin is irritated but not necessarily infected.
When a follicular infection sets in, the reading changes. The follicle becomes a small infectious focus. The lump is firmer. It is painful to touch, sometimes painful even without contact, with a feeling of tension. The skin is warmer locally. A white or yellowish spot can appear, a sign of pus. In some cases, the lesion turns into an inflammatory cyst. The lump is red, swollen, and feels “under the skin,” deeper than a surface bump.
Location helps too. An isolated bump on the leg after depilation does not have the same dynamics as a lesion on the pubis, exposed to friction and moisture. On the beard, repeated microlesions from shaving can encourage skin bacteria to enter the follicle. The infection usually stays local but can spread if the area is manipulated, pierced, or scratched.
Pigmentation is among possible sequelae. Repeated inflammation can leave a darker spot, especially on intermediate to dark phototypes. It is not dangerous, but it can take a long time to fade. Scratching and “picking” the crust increase the risk of lasting marks and depressed scars.
The most frequent temptation is to look for the hair with nails, tweezers, or a needle. The problem is not the intention, which is understandable. The problem is the path. An uncontrolled micro-opening can introduce germs, turning irritation into infection, then into an abscess. Even superficial disinfection does not sterilize a home needle nor the skin in depth. The action that seems “liberating” at the moment can complicate the aftermath.
| What is observed | Common interpretation | Suitable home response | When to seek advice |
|---|---|---|---|
| Small red bump, slight itch, mild pain | Inflammation related to a trapped hair | Gentle skin care, hydration, avoid shaving/depilation for 7 to 10 days | If it persists beyond 10-14 days or recurs in the same spot |
| Harder lump, warm skin, clear pain | Marked inflammation, possible early infection | Gentle cleaning, short local antiseptic, do not manipulate | If size increases in 24-48 h or if pain becomes throbbing |
| White/yellow spot, pus, spreading redness | Follicular infection or cyst | Do not pierce, cover if friction, avoid depilation | Consultation recommended, especially if fever or red streaks |
| Multiple lesions on pubic/armpit, recurring nodules | Favorable terrain, differential diagnosis to discuss | Limit friction, gentle hygiene, note triggering factors | If frequent recurrences, to rule out hidradenitis-like dermatosis |
A point deserves to be clearly named. Certain skin diseases, like hidradenitis suppurativa (often called Verneuil’s disease), can resemble infected ingrown hairs. The difference lies in repetition, depth of nodules, scars, and location in folds. A concerned parent or adult should not decide alone. A dermatologist can differentiate and propose an appropriate strategy.
An ingrown hair becomes worrying when pain rises rapidly, the lesion fills with pus, or several lesions appear in the same area. This guideline provides a simple compass without dramatizing. The logical next step is to discuss what can be done at home without worsening, and what requires professional care.
When the skin is irritated, choices in the next 48 hours often matter more than the “big dreamed solution.”
Ingrown hair treatment: safe home actions, disinfection, and situations requiring a professional
In most cases, ingrown hair treatment starts with patience and protection. The hair often eventually finds the surface on its own. This delay is frustrating, especially when the bump itches or the area is visible. The skin, however, needs calm to reduce inflammation. Repeated friction, shaving “to even out,” or tight clothing maintain the problem.
The first action is simple. Clean once a day with a gentle product, rinse, dry without rubbing. On a weeping or scratched area, a short local disinfection can help, with an appropriate cutaneous antiseptic. The aim is to limit bacterial proliferation, not to strip the skin. Harsh and repeated antiseptics dry and weaken, sometimes prolonging healing.
The second useful action is exfoliation, but it must be thought of as a gentle mechanical aid, not as abrasive scrubbing. Too coarse grains or too hard a brush can create microlesions, then additional inflammation. A gentle chemical exfoliation, such as low-concentration fruit acids, or a very fine scrub, 1 to 2 times per week, is often enough. It aims to thin the stratum corneum to allow the hair to pass.
Hydration comes just after. An emollient treatment makes skin more supple, reduces tightness, and helps hair exit. On the bikini area or armpits, non-occlusive textures are often better tolerated. Reactive skin appreciates short formulas without fragrance. Skin care is not a luxury in this context. It is part of the healing mechanism.
What to avoid, even when the urge is strong
Using a needle or tweezers to “go after” the hair seems logical. The skin, however, behaves like living tissue. A non-sterile opening can seed the area. The result can be a deeper infection, sometimes a cyst requiring medical drainage.
When the hair is visible under a thin skin layer, a professional can free it under clean conditions. They work with sterile material and make a tiny opening in the right spot to limit scarring risk. This difference in context changes everything. It’s not a question of courage, it’s a question of microbiology.
Local antibiotics and cyst: when care becomes medical
If an ingrown hair is accompanied by pus, marked pain, or a red swollen cyst, a doctor may prescribe a local antibiotic. This is an ointment or lotion applied for a specific duration. Using an antibiotic left over from another condition increases the risk of inefficacy and bacterial resistance. In 2026, this issue is even more sensitive than ten years ago because antibiotic resistance has become a well-documented public health concern.
Consultation box: concrete guidelines without alarmism
A medical consultation is indicated if a lump resembles an abscess, if the pain becomes intense, if redness spreads, if fever appears, or if several lesions recur in the same area (pubis, armpits, beard). A dermatologist is especially useful when recurrences are frequent or when healing leaves persistent nodules.
For further practical home solutions, with gentle and realistic options, the resource remedies and useful actions against ingrown hair helps structure a routine without multiplying products.
Particular vigilance is required when a lesion in the intergluteal fold or near the coccyx repeats and becomes infected. This picture can suggest a pilonidal cyst, which should not be confused with a simple ingrown hair. Specific information is available via understanding the pilonidal cyst in women.
The most protective rule is not to turn a bump into a wound. Then prevention is organized around simple gestures, chosen according to the skin, area, and depilation rhythm.
When the acute episode calms down, the skin becomes more receptive to adjustments that avoid repetition.
Ingrown hair prevention: choosing depilation, adjusting regrowth, and building a skin care routine
Ingrown hair prevention is not a fight against hair. It’s a compromise between aesthetics, comfort, and physiology. The first step is to look at the depilation or shaving method used, and how the skin reacts in the following 72 hours. Skin that burns, tingles, or breaks out in micro-bumps signals a barrier irritation. In this context, regrowth rarely happens “cleanly.”
When shaving is chosen, it benefits from preparation. A warm shower softens keratin. A shaving gel reduces friction. A blade changed regularly cuts cleaner. On the face, following the hair growth direction, even if the result is less “perfect,” reduces hairs curling under the epidermis. On the legs, avoiding multiple passes at the same spot limits invisible micro-cuts.
Regarding depilation, waxing pulls hair out, and regrowth can ingrow if the skin is thickened. Some people tolerate depilatory cream better, which dissolves the hair shaft without traumatizing the follicle, if strictly respecting the application time and testing on a small area. Others find a balance with an electric shaver, which cuts a bit higher and leaves fewer hairs “too short and pointy.”
A short and sustainable routine, especially when days are busy
An effective routine comes in few steps. It follows the regrowth rhythm. Care is most useful in the days following depilation, when the hair is seeking its path.
- Moisturize the skin after showering with a simple, well-tolerated texture, then continue for 3 to 4 days after depilation.
- Perform a gentle exfoliation 24 to 48 hours after depilation, then once a week if the skin tolerates it, without rubbing to redness.
- Reduce friction on risk zones for 48 hours, choosing looser clothing and breathable fabrics.
- Space out aggressive actions when bumps recur, even if the ideal aesthetic schedule is not followed.
Focus on sensitive areas: bikini, armpits, beard
In the bikini area, the skin is thin and reactive. Friction and heat increase inflammation. A soothing post-depilation care, fragrance-free, and cotton underwear often reduce reactions. On sports days, a quick shower after exercise decreases prolonged contact of sweat with the area, which limits the favorable terrain for follicular infection.
In the armpits, alcohol-based or heavily scented deodorants can irritate skin already weakened by shaving. Spacing application in the first days after shaving, or choosing a gentler formula, sometimes significantly improves tolerance. The beard requires attention to growth direction and blade quality. Regular maintenance of tools is part of care, just like moisturizing cream.
When ingrown hairs are very frequent, discussing more lasting options with a dermatologist may be relevant. Laser, for example, is not a universal answer. It depends on phototype, hair type, and pigmentation history. Personalized advice avoids overly quick promises and helps choose a realistic protocol.
Prevention relies less on a unique product than on coherence between depilation method, skin condition, and daily friction. This coherence gives skin that heals better and regrowth less trapped, which also lightens the mental burden associated with recurrences.
Can an ingrown hair go away on its own?
Yes, in most cases. When the skin sheds and the stratum corneum softens, the hair can regain the surface without intervention. Regular hydration and gentle, spaced exfoliation increase the chances of this happening without bumps or marks.
Should an ingrown hair always be disinfected?
Disinfection is not systematic. It becomes useful if the area has been scratched, if a small wound is present, or if the skin is weeping. An appropriate cutaneous antiseptic, used briefly, is often sufficient. Repeated and aggressive disinfection can dry out and delay skin healing.
How to know if it is a follicular infection?
Signs suggesting follicular infection include stronger and deeper pain, local heat, increasing swelling, appearance of pus (white/yellow spot), or redness spreading around the lesion. In such situations, it is better to avoid any manipulation and seek medical advice.
What exfoliation to choose to avoid ingrown hairs in the bikini area?
Gentle exfoliation is usually better tolerated than coarse grain scrubs. A light chemical formula (for example based on low-concentration fruit acids) or a very fine scrub, 1 to 2 times per week, helps limit surface thickening. If the area reddens or burns, exfoliation is too aggressive and should be spaced out or adjusted.
When to consult for recurring ingrown hairs?
Consultation is recommended if a red, painful cyst forms, if multiple lesions appear in the same area (pubis, beard, armpits), if pain becomes intense, if the lesion grows rapidly, or if fever is present. A dermatologist can also verify that it is not another fold disease, like hidradenitis, and propose appropriate treatment.