In brief
- Teething refers to the eruption process, whereas denture corresponds to the set of teeth present in the mouth at a given time.
- A tooth has a visible part, the crown, and an anchored part, the root, held in the bone by supporting tissues.
- The outer layer, the enamel, protects the tooth but does not regenerate once damaged.
- The 4 main families are the incisor, the canine, the premolar, and the molar, each with a distinct shape and masticatory role.
- The eruption of baby teeth often starts around 6 months and the temporary dentition is in place by about 2 and a half to 3 years, with frequent variations.
- Occlusion describes how the upper and lower teeth meet, impacting chewing, breathing, and sometimes pronunciation.
- Orthodontics may be proposed when alignment or occlusion interfere with function or risk damaging teeth, not just for aesthetics.
Understanding what a tooth is to better follow human teething
In the early years, many parents notice swollen gums, abundant saliva, a need to chew, sometimes more interrupted sleep. This picture often corresponds to teething, i.e. the biological process by which teeth break through the gum and take their place on the arch.
A tooth is a hard organ, implanted in the jaw bones. It appears small, white, simple. In reality, it is made up of specialized tissues, crossed by microcanals and connected to a nervous and vascular network that explains why toothache can become very overwhelming, even when the lesion is minimal.
Clear dental anatomy, without unnecessary jargon
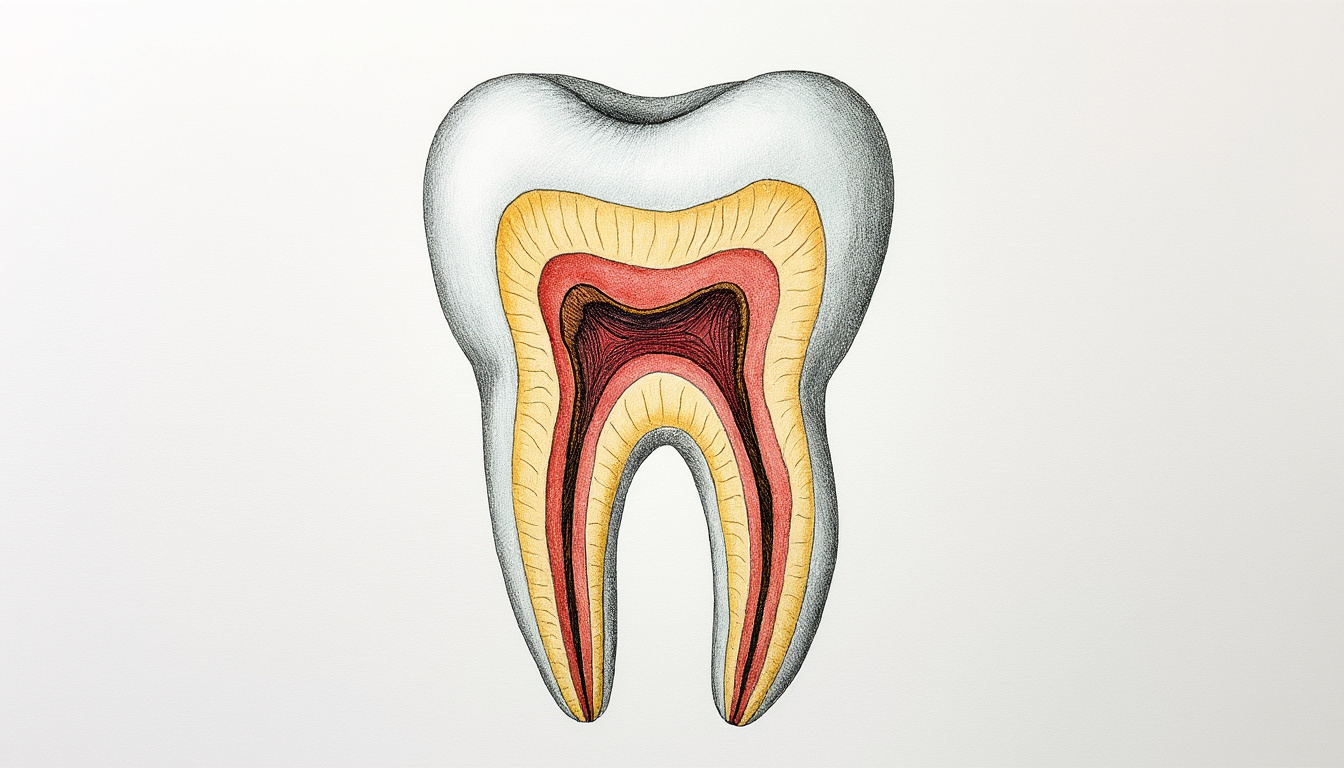
The first useful distinction is between the visible part and the hidden part. The crown is what protrudes from the gum. The root is the part anchored in the bone, invisible but decisive for stability.
The crown is covered with enamel, a highly mineralized layer, designed to withstand the friction of chewing. Enamel protects but does not “regrow.” When weakened by a cavity, acid erosion, or trauma, the underlying tissue becomes more exposed.
Below the enamel lies the dentin. It is less hard, more sensitive, crossed by tubules that can transmit sensations of cold, sweetness, or brushing. At the center, the pulp contains nerves and vessels. When inflammation reaches this area, the pain often becomes throbbing, sometimes nocturnal, because internal pressure increases and the nerve is highly reactive.
Why teeth “react” so much in children
The perception of discomfort is modulated by the immaturity of the nervous system and the fact that the baby does not yet have strategies to relieve themselves. Chewing, sucking more often, asking to be held, waking up more frequently is not a tantrum. It is a regulation attempt.
A simple guideline helps to sort this out: teething discomfort fluctuates throughout the day, with peaks, whereas continuous and worsening pain deserves medical advice. A locally swollen gum and a need to chew fit the usual scenario. Persistent high fever, marked drowsiness, refusal to drink, or pain preventing sleep for several consecutive nights justify a consultation.
The logical next step, after anatomy, is to understand which teeth arrive, in what order, and what this changes in the mouth over months and years.
Ages, order of appearance, and number of teeth from child to adult
The number of teeth changes with age, and this often reassures. A child is not “missing” teeth because they have fewer. They follow a chronology. The temporary dentition most often has 20 teeth. The permanent dentition can go up to 32 teeth, depending on the presence or absence of wisdom teeth.
Teething of baby teeth often starts around 6 months. Variability is wide. Some babies cut a first incisor at 4 months, others at 10 months, without this indicating a problem if overall growth is harmonious.
Usual chronology of baby teeth, then permanent teeth
The most frequent sequence starts with the incisors, then the canines, and finally the molars of milk. The temporary dentition is generally complete around 33 months, often ranging from 2 and a half to 3 years.
Around 6 years, a transition starts. The first baby teeth fall out, often the incisors, and permanent teeth appear. The “mixed” period can surprise, with sometimes two visible rows. A permanent tooth that emerges behind a still-present baby tooth is fairly common. It is monitored without dramatization. If the baby tooth does not move while the permanent tooth is already well out, a dental opinion helps avoid overcrowding.
Most children have all their permanent teeth, excluding wisdom teeth, by around 12-13 years old. The third molars, called wisdom teeth, may erupt between 16 and 25 years, with significant variability. They can remain impacted, partially erupt, or never appear.
Table of teething and denture milestones
| Stage | Most common age | What you observe | When to seek advice |
|---|---|---|---|
| First baby teeth | Around 6 months (wide variation) | Sensitive gums, salivation, chewing, erupting incisor | Refusal to drink, persistent high fever, deterioration in general condition |
| Complete temporary dentition | Around 2 and 1/2 to 3 years | 20 teeth in place, more effective chewing | Early visible cavities, recurring pain, frequent gum bleeding |
| Start of permanent dentition | From 6 years old | Falling incisors, appearance of new teeth | Persistent double row, difficulty chewing, very tight teeth |
| Permanent dentition (excluding wisdom teeth) | Around 12-13 years | Alignment stabilizing, sometimes orthodontic treatment | Joint pain, abnormal wear, troublesome occlusion |
| Wisdom teeth | 16-25 years | Inflamed rear gums, pressure, possible lack of space | Repeated infections, pain, cyst, impact on neighboring teeth |
The practical thread to keep in mind sums up in one sentence. Teething is a succession of phases, and most age variations remain normal as long as the child eats, grows, and develops regularly. The next step is to understand the function of each type of tooth, which helps give meaning to their shape and place.
A clear video, delivered by a professional, can help visualize the order of appearance and spot what is a normal variation.
Incisor, canine, premolar, molar: functions and role in chewing
The mouth is not only for “having pretty teeth.” It serves to cut, tear, grind, swallow safely, and prepare digestion. Each tooth shape corresponds to a task. When a tooth is damaged or when occlusion is disturbed, chewing becomes less efficient. This may lead to swallowing faster, preferring soft textures, or tiring during meals.
The 4 types of teeth and what they really do
The incisor is shaped like a small blade. It cuts. It is often the first visible in photos because it appears early and marks the smile.
The canine has a more pointed tip. It tears. It also stabilizes the arch during lateral jaw movements. When a canine is very high or forward, it may change contacts and cause wear on neighboring teeth.
Premolars, present in permanent dentition, begin the grinding work. In children, they replace some baby molars. This substitution often surprises. A “baby molar” does not become a premolar. It falls out, and a premolar takes its place.
The molar is the large grinding surface, with reliefs designed to crush. It works with its “twin” above or below. When these contacts are not proper, occlusion is said to be disturbed. Some people then chew mostly on one side, which can generate muscle tensions.
Concrete example on a bite of bread, without oversimplifying
The sequence is quite constant. Incisors cut the first portion. Canines help tear the crust if needed. Premolars and molars then take over to reduce into smaller particles. Saliva begins starch digestion, then the food bolus is swallowed.
A child who has just cut a molar can chew more efficiently than a child who only has incisors. It’s not a question of “willpower.” It’s mechanical. This helps understand why some foods pass very well at one period, then become difficult for a few weeks during teething, before becoming accepted again.
When function alerts more than aesthetics
A tooth that grows a bit crooked can correct itself with growth. A frankly crowded alignment, a crossbite, or a misalignment that prevents closing the mouth properly justifies a consultation. Orthodontics is not just about “perfect” alignment. It aims to protect teeth, improve function, and distribute chewing forces.
This understanding of roles prepares well for what comes next. When teeth meet, occlusion is established. And when occlusion is not harmonious, certain signs appear daily.
Seeing jaw movements in images helps understand why a dental contact can influence chewing and sometimes comfort.
Occlusion, jaw growth, and orthodontics: practical markers for families
Occlusion describes how the upper and lower teeth fit together when the mouth closes. A balanced occlusion distributes forces. An unbalanced occlusion concentrates pressure on certain teeth, favors wear, and can sometimes cause muscle or joint pain, especially during adolescence when growth is rapid.
In children, jaws grow, teeth are replaced, the tongue finds its place. Variations are numerous. A space between baby teeth can be good news. It sometimes signals future room for larger permanent teeth.
Everyday signs that deserve professional attention
A consultation is not reserved for extreme situations. It allows measurement, observation, and deciding whether to act now or just monitor. A reassuring guideline is to look for functional signs, not just aesthetic ones.
- Persistent unilateral chewing with refusal to use one side, apart from a temporary teething episode.
- Visible wear on certain teeth, or repeated small fractures on an incisor.
- Mouth often open at rest, frequent snoring, mouth breathing, which can influence facial growth.
- Teeth that strongly overlap with difficulty in brushing, as caries prevention becomes more complex.
An orthodontic appliance is not systematic. Sometimes simple monitoring is enough. Sometimes an early interceptive treatment is offered to guide growth, widen an arch, or correct a crossbite. The benefit is then functional, and timing matters.
A often neglected point: gum health around moving teeth
Gums that bleed when brushing are not “normal” in the sense that they should be ignored. In children and adults alike, bleeding often indicates inflammation related to plaque. When teeth are crowded or during orthodontic treatment, hygiene becomes more technical. This does not mean more punitive. It means more guided.
A soft brush, a movement with small strokes close to the gum, and adapted interdental tools can change the outcome. A dentist or orthodontist can show the correct brushing angle in a few minutes, which is better than a vague injunction to “brush better.”
Consultation box: when not to wait
A rapid opinion is justified if pain wakes one at night for several consecutive days, if a gum swells significantly with discharge, if a tooth turns grey after trauma, or if chewing becomes impossible. In toddlers, mouth lesions can also be related to a non-dental cause. A white tongue and patches that do not go away with cleaning may indicate thrush, and a useful guide is here white tongue in infants and thrush.
If the mouth is affected from birth, for example in case of cleft lip and palate, feeding, growth, and later dentition require specialized support. A structured resource to understand this journey exists here cleft lip and palate in newborns.
The next step is even more concrete. Preserving enamel, limiting cavities, and making brushing feasible in real family life directly changes the teething experience daily.
Care, prevention, and small myths about teeth: protecting enamel without rigidity
Daily dental care often hinges on repetitive details. Technically correct brushing, attention to sugary drinks, rapid reaction to pain, and regular check-ups greatly reduce the risk of cavities. This applies as much to baby teeth as to permanent teeth.
Baby teeth matter. They guide the eruption of permanent teeth, maintain space, enable effective chewing, and contribute to comfort. A cavity on a temporary tooth can cause pain, infection, and sometimes affect sleep and eating. It is not a detail.
Realistic gestures for a child’s mouth
Brushing starts as soon as the first tooth appears. At first, a few seconds are enough to establish the habit. Gradually, the goal becomes a gentle real friction of all accessible surfaces. Adult presence is often necessary until 6-8 years for effective brushing, because fine motor skills and consistency are not yet stable.
A simple guideline helps: aim for two brushings per day, including a more thorough one in the evening. At night, saliva decreases during sleep, which reduces natural protection against acids. This is also why sugary snacks after evening brushing increase the risk of cavities.
Chocolate, fluoride, and what this really means
Cocoa contains minerals like fluoride and phosphate, which can help protect enamel. This does not turn chocolate into dental care. Dark chocolate, consumed as part of a meal, is generally less problematic than a succession of sticky sugars taken continuously. What harms enamel most is repeated acid attacks, more than occasional quantity.
Sugary drinks, juices, and slow-sipped pouches expose enamel to acids for prolonged periods. A good strategy is to reserve these intakes to mealtimes, then offer water afterward. It’s practical and avoids turning the day into constant negotiation.
Some historical markers, because prevention has built up over time
Toothbrushes have existed for several centuries. They appeared in China in the 15th century, then spread to Europe in the following century. Materials changed. Boar bristles were replaced by nylon in the mid-20th century, improving accessibility and brush hygiene. Today, the question is more about technique and consistency than the object itself.
Certain civilizations also modified teeth for aesthetic or symbolic purposes. The Mayas, for example, inlaid stones on the visible surface of teeth about 2500 years ago. This recalls a useful idea. Teeth are hard but not indestructible. Drilling, cracking, or grinding always has a biological cost.
When lifestyle habits affect toddlers’ safety
Oral prevention is also linked to overall safety. Trauma can break a baby incisor or a permanent tooth. Falls are more frequent when the child is placed in a device that does not respect their motor development. A useful read on this subject is here risks related to walkers, as teething is also protected by avoiding trauma.
Remaining attentive to pain, gum condition, and how the child chews allows early action without excessive worry. The rest are the questions that come up most often, the ones that save time and peace of mind daily.
What is the difference between teething and denture?
Teething refers to the biological process of tooth eruption. Denture refers to the set of teeth present in the mouth at a given time, for example the temporary denture of 20 teeth in children or the permanent denture which can go up to 32 teeth in adults.
At what age does the first tooth come out, and when are all baby teeth present?
The first tooth often appears around 6 months, with a normal variation of several months depending on the child. The baby denture is generally complete around 2 and a half to 3 years. An isolated delay is not necessarily worrying if growth and nutrition go well.
Is a permanent tooth erupting behind a baby tooth serious?
It is common during the transition period. The baby tooth often mobilizes and falls out. A dental opinion is useful if the baby tooth remains fixed, if the child has pain, or if the double row persists for several weeks with significant crowding.
What signs should prompt a rapid consultation for tooth pain?
Pain that wakes the child repeatedly at night, severely swollen gum with discharge, a tooth that changes color after trauma, refusal to drink or deterioration of general condition justify rapid consultation. In toddlers, mouth lesions can also be due to an infectious cause, hence the interest in evaluation if symptoms persist.
What is the purpose of orthodontics if teeth just seem a little crooked?
Orthodontics often aims at function. It can improve occlusion, distribute chewing forces, limit wear, and facilitate hygiene when teeth are very crowded. The decision is made case by case, taking into account growth, crowding, and functional signs (chewing, wear, tension).